

You don’t have to accept intrusive thoughts or rituals as part of daily life; effective treatments can reduce symptoms and improve functioning. Exposure and response prevention (ERP) therapy and certain medications like SSRIs are the primary, evidence-backed options that most people find helpful.
This article explains how those treatments work, what to expect from therapy and medication, and how to choose the right approach for your situation. You’ll get practical guidance on identifying skilled providers and next steps so you can start making informed decisions about care.
Overview of OCD Treatment
OCD Treatments targets unwanted thoughts (obsessions) and repetitive behaviors or mental rituals (compulsions). Effective options include specialized therapies, medications that adjust serotonin, and often a planned combination tailored to your symptoms and response.
Types of Therapies
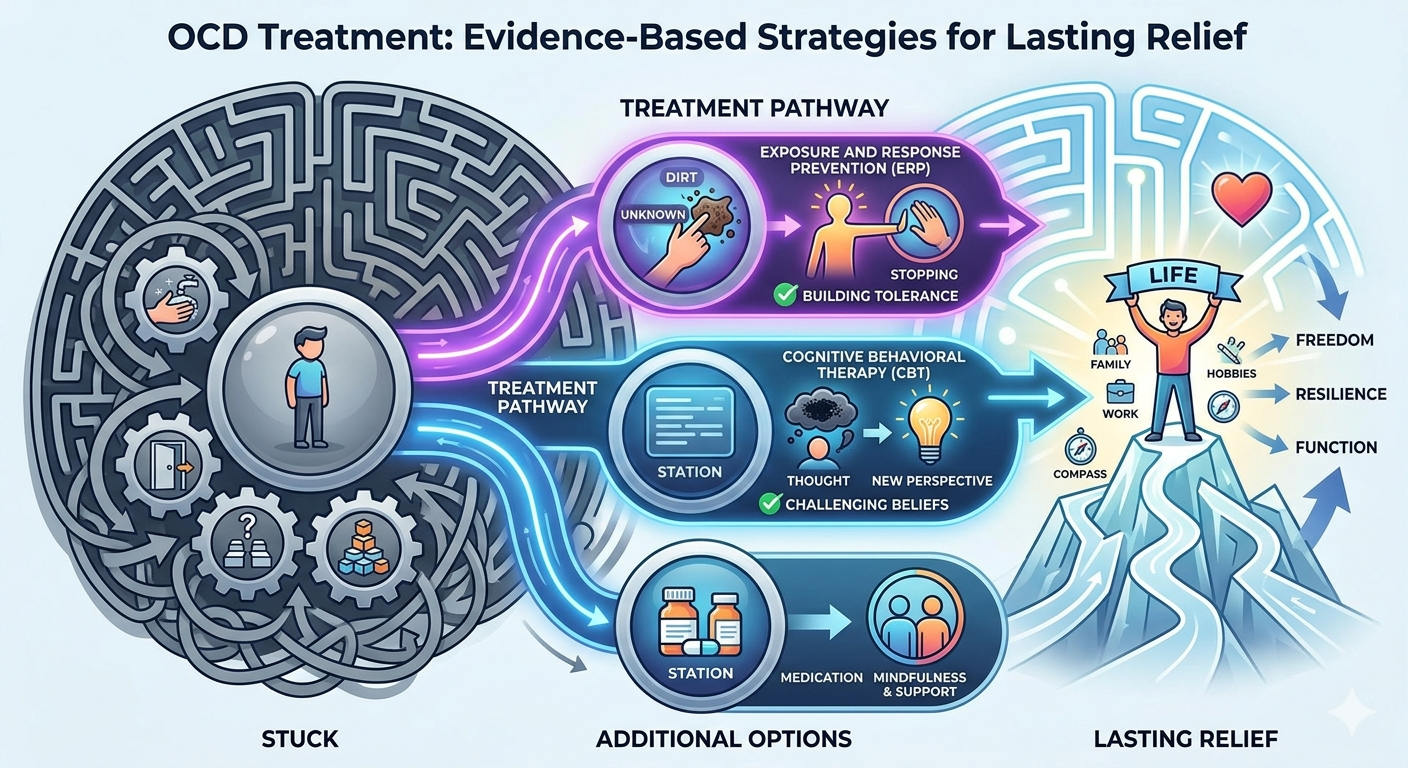
The most evidence-based therapy is cognitive behavioral therapy (CBT) with exposure and response prevention (ERP). In ERP you intentionally confront feared thoughts or situations and then refrain from the ritual; repeated practice reduces anxiety and weakens the obsession–compulsion cycle. Sessions usually occur weekly with homework exercises; progress depends on gradual, consistent exposures.
Other psychotherapies can help when ERP alone is insufficient. Cognitive therapy targets the thinking patterns that fuel obsessions. Acceptance and commitment therapy (ACT) and mindfulness-based approaches teach skills to tolerate distress without acting on compulsions. Intensive or residential programs provide daily ERP if symptoms severely limit functioning.
Medications for OCD
First-line medications are selective serotonin reuptake inhibitors (SSRIs) at higher doses and often longer trials than for depression. Common choices include fluoxetine, sertraline, fluvoxamine, and higher-dose escitalopram or paroxetine. Expect 8–12 weeks to assess response; dose adjustments may follow.
When SSRIs give incomplete relief, clinicians may try clomipramine, an older serotonin-focused tricyclic, or augment SSRI treatment. Augmentation options include low-dose antipsychotics for certain symptoms, guided by specialist assessment. Monitor side effects, interactions, and suicidal thinking, especially when starting or changing doses.
Combination Approaches
Combining CBT/ERP with medication often yields faster and larger symptom reduction than either alone for many people. You might start medication to reduce anxiety enough for ERP to be tolerable, or begin ERP first if you prefer nonpharmacologic care.
Multidisciplinary plans coordinate psychiatrists, therapists, and primary care to adjust therapy intensity and medication. For treatment-resistant cases, options include intensified ERP, medication optimization, augmentation strategies, and referral for neuromodulation (e.g., rTMS or deep brain stimulation) in specialized centers.
Choosing the Right OCD Treatment
You should focus on treatments proven for OCD and on practical factors you can control: symptom type and severity, treatment availability, and your preferences. Prioritize options with strong evidence, like ERP and SSRIs, and plan how you’ll track progress and adapt if needed.
Factors Affecting Treatment Selection
Assess your symptoms precisely: note whether intrusive thoughts, checking, contamination fears, or mental rituals dominate. Symptom type affects therapy choice—ERP targets behavioral rituals and avoidance, while cognitive approaches help with unwanted thought patterns. Measure severity and functional impact; severe, suicidal, or highly disabling cases often require combined medication plus therapy and faster specialist referral.
Consider comorbid conditions such as depression, bipolar disorder, or substance use. Medication choices differ if you have bipolar disorder or pregnancy concerns. Practical constraints matter: therapist availability, insurance coverage, cost, and your ability to attend regular sessions. Finally, weigh your readiness for exposure work—ERP demands repeated, often uncomfortable practice. If you’re unwilling or unable to do ERP, discuss alternative or adjunctive approaches with your clinician.
Working with Mental Health Professionals
Choose clinicians experienced in OCD-specific treatments. Look for therapists trained in Exposure and Response Prevention (ERP) and clinicians comfortable prescribing higher SSRI doses used for OCD. Ask about case volume: therapists who treat OCD regularly tend to apply ERP more effectively.
Set concrete goals and a treatment plan with milestones and timelines. Confirm the therapist’s ERP approach (in vivo, imaginal, or combined), session frequency, homework expectations, and relapse prevention strategies. If medication is recommended, ensure the prescriber monitors dose adjustments and side effects closely. Consider a multidisciplinary team—therapist, psychiatrist, and primary care provider—when symptoms are complex or treatment-resistant.
Monitoring Progress and Adjustments
Track symptoms with objective tools like the Yale-Brown Obsessive Compulsive Scale (Y-BOCS) or weekly symptom logs. Record frequency, distress level, time spent on rituals, and impact on daily functioning. Review these measures with your clinician every 4–12 weeks to judge response.
Expect adjustments: increase SSRI dose, switch medications, intensify ERP, or add augmentation options if improvement is limited after an adequate trial (usually 8–12 weeks for medication). For partial responders, consider adding CBT components, acceptance-based strategies, or specialist referral for neuromodulation or consultation. If side effects, life events, or adherence issues emerge, address them promptly to avoid stalled progress.







